
World Malaria Day was observed recently and each year at this time, conversations tend to focus on progress — declining incidence rates, global eradication targets, and long-term public health milestones. While it is important to acknowledge the increased visibility this has brought to malaria control efforts and the advances in research and treatment, there is a growing concern that the narrative is becoming too abstract.
In doing so, we risk losing sight of what is still happening on the ground: malaria has not become less dangerous. If anything, its outbreaks have become more predictable, yet responses remain dangerously delayed, particularly in underserved communities where access to timely care is based of finance.

The World Health Organization estimates that malaria still causes over 200 million cases annually, with more than 600,000 deaths each year, and about 94% of those deaths occurring in Africa, predominantly among children under five. UNICEF continues to highlight malaria as one of the leading causes of preventable childhood mortality on the continent. These are not historical figures. They are the current realities.
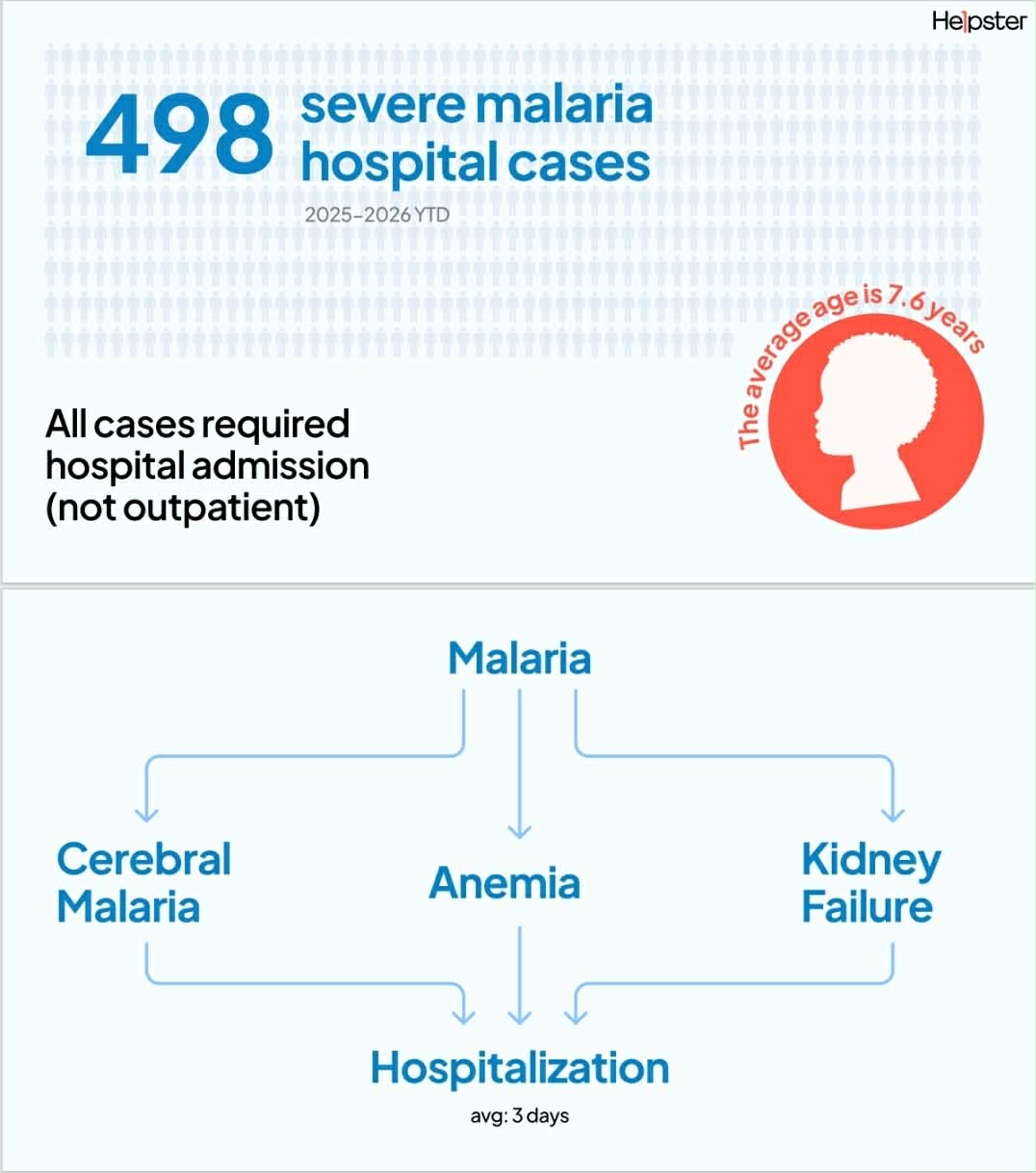
At Helpster Charity, between 2025 and 2026 to date, we supported 498 severe malaria cases requiring hospitalization. These were not mild or early-stage cases. Every patient in this cohort had already crossed into clinical severity — requiring urgent admission rather than outpatient treatment. The average age of these patients is 7.6 years, a figure that should immediately sharpen our understanding of where the burden is concentrated: children who depend entirely on the timing of adult decisions, access to care, and affordability.
We also recorded cases involving pregnant women, including women in their early thirties, where malaria becomes not just an individual illness but a dual-risk condition affecting both mother and unborn child. In these situations, the consequences are intergenerational and far more complex than a single infection episode.
These cases rarely exist alone. The most common complications we see include cerebral malaria, anemia, and kidney failure. Malaria acts as the trigger, but what unfolds is a wider clinical collapse shaped by delayed care-seeking, underlying vulnerability, and systemic gaps in early intervention. Most patients are hospitalized for an average of three days, but those three days are often preceded by much longer periods of unmanaged fever at home, where families delay seeking care due to cost constraints or uncertainty about severity.

The financial reality is equally revealing. Across these cases, the average treatment cost is approximately $82.50, with extremes ranging from $15 to $560, depending on complexity. While these figures may appear modest in global health discussions, they are significant in the context of the households affected. Importantly, treatment is always initiated immediately at Helpster-supported facilities, before payment is resolved, because in severe malaria, delay is not clinically acceptable. Yet administrative confirmation of cases often takes between two weeks and one month, reflecting a persistent gap between urgent clinical response and slower institutional documentation systems.
Malaria is also highly seasonal, and our data reflects clear clustering during and after rainy periods, with peaks consistently observed in May, June, October, and November. This is not new epidemiological knowledge. What remains unresolved is the implication of that predictability. Each year, the same seasonal conditions produce surges in severe cases, yet the preparedness of households and systems does not scale in proportion. Predictability without resilience simply becomes repetition.
A further complexity lies in financing. Our intake system focuses on patients who cannot independently afford care, meaning every case represents not just a medical emergency but a financial one. In this context, conventional ideas around micro-credit or repayment capacity become difficult to apply meaningfully. In the middle of a child’s fever crisis, the question is not repayment structure — it is survival and immediacy of access.
Within this cohort, luckily, we have no confirmed malaria-related deaths recorded based on available partner reporting and case management data. While this is encouraging, it should not be misread as evidence that risk is absent.
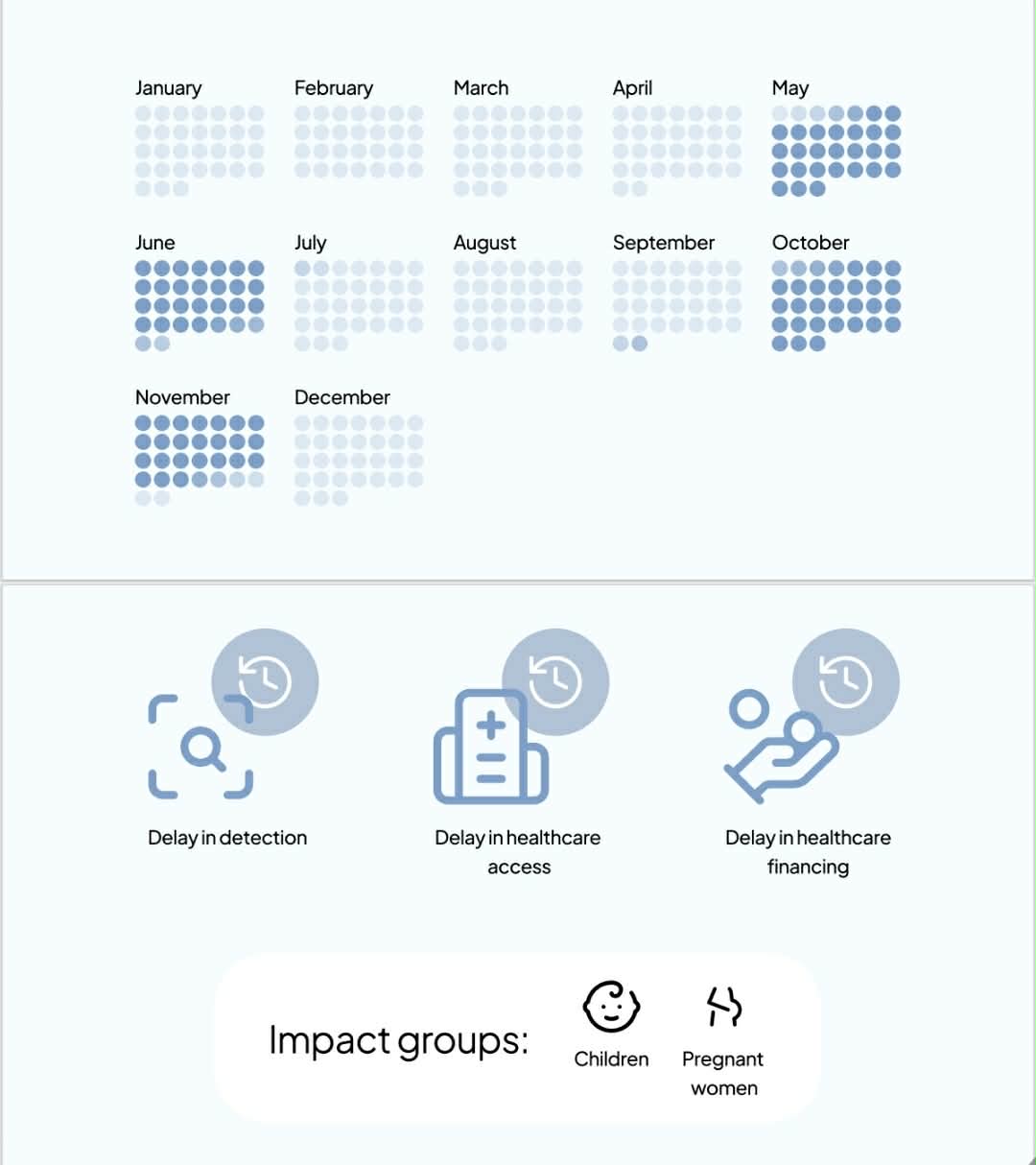
What emerges clearly from this data is that malaria is no longer simply a disease of incidence. It is a disease of delay — delay in detection, delay in care-seeking, delay in financing, and delay in system coordination. It disproportionately affects young children and pregnant women, who have the least capacity to withstand these delays. And its true burden is not captured by infection numbers alone, but by the complications, comorbidities, and systemic inefficiencies that turn preventable illness into hospitalization.
A child admitted for three days of inpatient care is not just a clinical case. It is an indicator of earlier failures — in prevention, in access, or in affordability. When nearly 500 such cases are recorded through one organization in just over a year, the question is no longer if malaria remains a public health challenge. The question is why severity is still the entry point into care.
World Malaria Day must move beyond symbolic recognition and confront a harder truth: progress cannot be measured by declining incidence alone when preventable infections are still escalating into emergencies. Until early detection, timely access to care, and financing mechanisms operate with the same urgency as the disease itself, malaria will remain not something we are eliminating, but something we are repeatedly forced to manage at its most severe and costly stage.
For the children and families behind these numbers, intervention after deterioration is not enough. At Helpster Charity, our work is rooted in closing that gap — continuously refining our systems to reach underserved communities earlier and ensure that lack of funds never delays lifesaving care. Our goal is simple: make access to quality healthcare immediate, efficient, and dependable when it matters most.
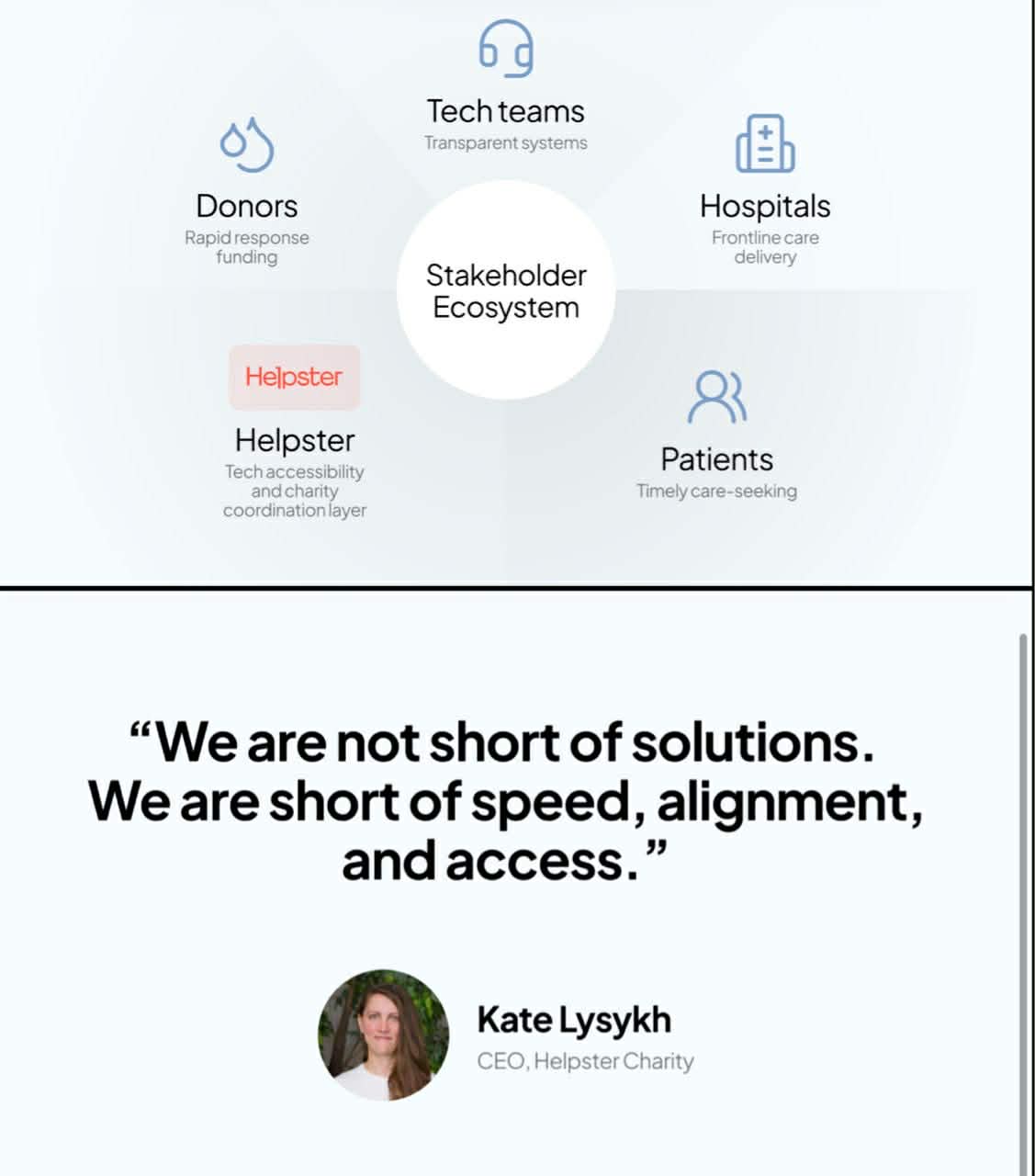
But no single organization can solve this alone. Real progress depends on a collective effort; from donors who enable rapid response, to technology teams building transparent and efficient systems, to healthcare partners delivering critical care, and even to the patients and families who take the step to seek help. Ending malaria, and other treatable conditions like it, will require that shared commitment to act earlier, faster, and together.
By Kate Lysykh, CEO, Helpster Charity.